We have coached hundreds of aspiring diagnostic medical sonographers, clinical ultrasound technicians, and cross-training radiologic technologists through this milestone ARDMS Abdomen certification. Let's look honestly at the modern healthcare credentialing landscape. The medical professionals who fall short on this rigorous, 170-question specialized evaluation are almost always those who leaned heavily on low-quality, linear test pools—those flat, context-stripped answer repositories floating around unverified internet forums. Those static, unverified materials simply cannot prepare you for live patient artifact identification or the complex pathology adjustments tested on the real exam. Candidates frequently get stuck looking for high-yield AB Abdomen exam questions online, trying to locate realistic ARDMS Abdomen Sonography practice tests to measure their diagnostic logic, or hunting for an updated AB-Abdomen study guide that breaks down advanced Doppler spectral analysis. They quickly discover that rote memorization fails completely when faced with complex, scenario-based congenital anomaly classifications and real-time hemodynamic changes.
At Exact2Pass, our framework targets the underlying structural logic, scanning physics, and clinical evaluation rules of the active American Registry for Diagnostic Medical Sonography curriculum instead. Our premium preparation platform delivers comprehensive diagnostic breakdowns for every structural anomaly and vascular flow velocity pattern. You will master actual core clinical execution rules instead of leaning on short-sighted memorization shortcuts. We map out hepatic multi-tier vascular systems, acoustic shadowing and enhancement variables, Transjugular Intrahepatic Portosystemic Shunt (TIPS) performance monitoring, and renal parenchymal echogenicity shifts step by step. Our learning material is designed from the ground up by active, registered sonographers and clinical instructors who orchestrate actual hospital scanning suites daily. Because of that, we completely avoid mindless, repetitive question lists. Instead, our software acts as an active clinical simulation that forces you to evaluate scan planes, adjust time gain compensation (TGC) levels, and isolate subtle retroperitoneal patholgoies like a veteran sonographer. You will learn the exact reason why a specific probe positioning or Doppler optimization technique succeeds or drops critical diagnostic detail. That is how you build real confidence before logging into your official ARDMS dashboard or scheduling your seat at a Pearson VUE professional center. Our adaptive software environment develops deep diagnostic mastery that transfers perfectly to live clinical rounds, helping you pass on your very first try.
A patient with hepatocellular carcinoma presents for a paracentesis. Which lab value is the most pertinent to the procedure?
Which description is associated with the normal sonographic appearance of a tendon?
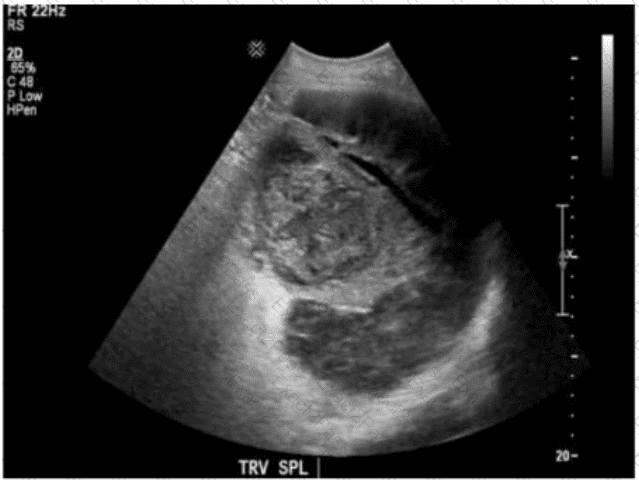
Which clinical finding is most likely associated with the splenic pathology demonstrated in this image?
Which finding is an indication for renal biopsy to assess for renal failure?
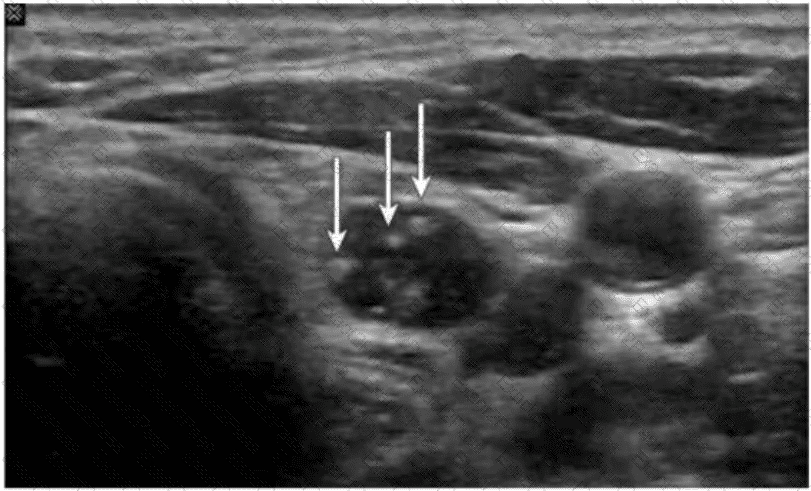
Which condition is most consistent with the sonographic appearance indicated by the arrows on this image obtained post thyroidectomy?
Which gray scale artifact is caused by the oscillation of gas bubbles?
Which is the most common pancreatic cancer?
Which condition is a cause of intrahepatic dilatation with a normal common bile duct?
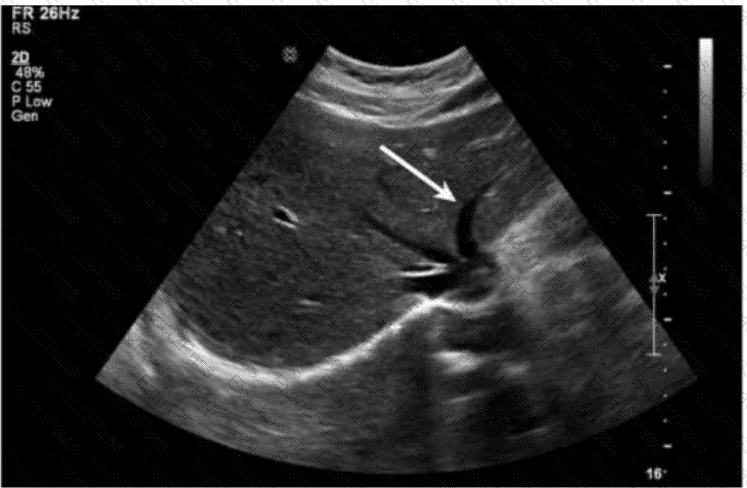
Which sections of the liver are divided by the structure indicated by the arrow on this image?
Which lymph node shape is concerning for malignancy in the post-thyroidectomy neck?

